**** I am not a health care professional nor do I have anything that looks remotely like a medical degree. So take anything I say with a pinch of salt.
For this piece I have combined information I found on; Diabetes Daily written By Ginger Vieira on January 4th, 2016, from Beyond Type 1 WRITTEN BY: Kyla Schmieg, BSN, RN and from The Type 1 Diabetes Network Australia Type 1 Diabetes Starter Kit
When I was diagnosed in 1993, I don’t remember hearing the word ketone back then. In fact, I don’t think I hear it until the early 2,000’s. Remember, diabetes education didn’t exist in Ireland before then - not to my recollection anyway.
In my 23 years with type 1 diabetes I have never tested for ketones. Firstly I don't often get sick. And secondly, when I’m sick I take all the recommended actions that deal with both being sick and flushing out ketones.
 However, I hear a lot of talk about ketones and began to think that, maybe, I'm a bit too relaxed about them and need to know a bit more.
However, I hear a lot of talk about ketones and began to think that, maybe, I'm a bit too relaxed about them and need to know a bit more.
So, first, what is a ketone?
When our body can’t access glucose, it looks to burn fat for energy. Burning fat results in ketones.
“Ketones build up can lead to Diabetic Ketoacidosis (DKA). Signs of DKA include nausea, vomiting, abdominal pain, fruity or acetone (think nail polish remover) breath, rapid breathing, flushed skin, and lack of energy.“ http://beyondtype1.org/ketones-the-6-must-knows/
Why are they so scary?
Ketones usually build up in a person with diabetes if they do not have enough insulin taken and can be fatal.
If ketones happen “too much too fast, it is not natural and it’s important to understand that ‘normally’ produced ketones are very different from ketones that develop due to insulin deficiency.
Moderate or large amounts of ketones in your body are very dangerous. They upset the chemical balance of the blood and lead to a condition called diabetic ketoacidosis or DKA. Some people also experience fast and heavy breathing and exaggerated beating of their heart. It is scary! If you experience DKA, you need to go to hospital to be rehydrated and monitored while the ketones in your body reduce to a safe level.
Many people with type 1 diabetes have never had an episode of ketoacidosis, but you may have already experienced DKA during diagnosis. Unfortunately, DKA is life threatening, so you need to understand what it is and what to look out for.” (from the Type 1 Diabetes Network’s Starter Kit page 37)
OK, I’ve got it so far.
This much is easy to follow but when I started hearing about the different type of ketones that were I got a bit lost. Especially when I heard that you can have ketone when you are not sick and have normal blood sugar levels. Until I did this research, I didn’t know if that was a “freak-out” or “not-to-freaky-out” situation.
Different types of ketones.
Illness-Induced Ketones
Illness-induced ketones can be very dangerous for a person with any type of diabetes. People with diabetes who are sick, especially with an infection, a stomach bug, or the flu should always test their ketones while they are sick.
A mild illness can cause low level ketones that are usually not life-threatening or severely serious. If ketones are at low levels, the general suggestion is to consume plenty of fluids and talk to your healthcare team about increasing your background insulin doses.
Even if your blood sugars appear in-range but you are producing ketones when sick, an increase in background insulin can help eliminate the ketones without dropping one’s blood sugar.
On the other hand, a person with diabetes, who is vomiting repeatedly will almost always need to get to the ER as quickly as possible. Vomiting, no matter the cause of the vomiting, will likely induce large ketones and can be life-threatening. Vomiting leads to severe dehydration which will escalate ketones further to a state of DKA.
Since severe ketosis will likely make a person extremely nauseas in addition to their illness-induced nausea, it can be nearly impossible to consume enough fluids at home to re-hydrate the body. An IV drip of saline at the hospital is essential to rehydrating the body, reducing or eliminating ketones, and stabilizing blood sugar levels.
Consult your healthcare team if you have concerns about your state of ketosis.
Starvation Ketones
Starvation ketones are simply the result of not eating enough food over the course of several hours. Both diabetics and non-diabetics can easily produce very low levels of ketones overnight, seeing a faint pink color on a urine ketone strip first thing in the morning. These are not dangerous unless, of course, this person continues to starve themselves.
Nutritional Ketones
Nutritional Ketosis is a state where the body is using ketones as a fuel source efficiently and safely. In individuals without diabetes or in those with controlled diabetes, having insulin on board to maintain healthy blood sugar levels keeps ketone production in the safe range.
This is achieved by reducing carbohydrate-intake to below 50 grams, because when glucose from food is limited, but blood sugars are still in a healthy range and enough insulin is present, the body will begin to burn body fat for fuel instead, producing low levels of ketones in the bloodstream.”
As long as blood sugars are maintained in the normal safe range with insulin, someone with diabetes can very safely be in Nutritional Ketosis.
When you’ve been in Nutritional Ketosis and not even known it:
- when you skip breakfast and don’t eat until lunch or later, your body is burning body fat for fuel and likely producing low-levels of ketones
- when babies are born, they are often in a state of nutritional ketosis for the first few days or week of life because they are consuming very little breast milk until the mother’s breast milk production ramps up
- when you eat a low-carb meal (eggs and bacon) for breakfast and don’t eat again until late lunch or afternoon…or…when you eat a low-carb breakfast followed by a low-carb lunch, your body is producing a low level of ketones until you eat a more significant serving of carbohydrates at dinner, etc.
Can you get ketones with a high blood sugar?
Ketones typically accompany high blood sugar. Ketones indicate your body needs more insulin. Most often if your body needs more insulin, it means your probably have a high blood sugar. Also, when an illness is present, your body releases hormones in response to the stress. These hormones lead to elevated blood glucose. That is why it’s recommended to test ketone levels during illness.
Can you get ketones with a normal or low blood sugar?
Ketones can also be present when your blood sugar is normal or low. These are sometimes referred to as “starvation ketones” or “nutritional ketosis.” During an illness or extreme diet change, if you have a significant decrease in carb intake, this can lead to the body using fat for energy because there are not enough carbs present to burn. Your blood sugar could remain normal or even be low in this case but your body could still be producing ketones.
From; http://beyondtype1.org/ketones-the-6-must-knows/
Conclusion
My conclusion is that, like diabetes, ketones need to be treated seriously. They are not always scary but you need to know why, when and how. And remember, if in doubt call your D-team. A quick phone call equals peace of mind.
Sources of information about ketones;





 I am very excited about attending this conference to meet other diabetes bloggers and advocates from all over Europe. I’ve already connected with some of the them through twitter. But also I’m excited because unlike other company blogger events the agenda for this one is about helping us become better at what we do without it costing our own personal health. This is something I have struggle with for a couple of years now.
I am very excited about attending this conference to meet other diabetes bloggers and advocates from all over Europe. I’ve already connected with some of the them through twitter. But also I’m excited because unlike other company blogger events the agenda for this one is about helping us become better at what we do without it costing our own personal health. This is something I have struggle with for a couple of years now.
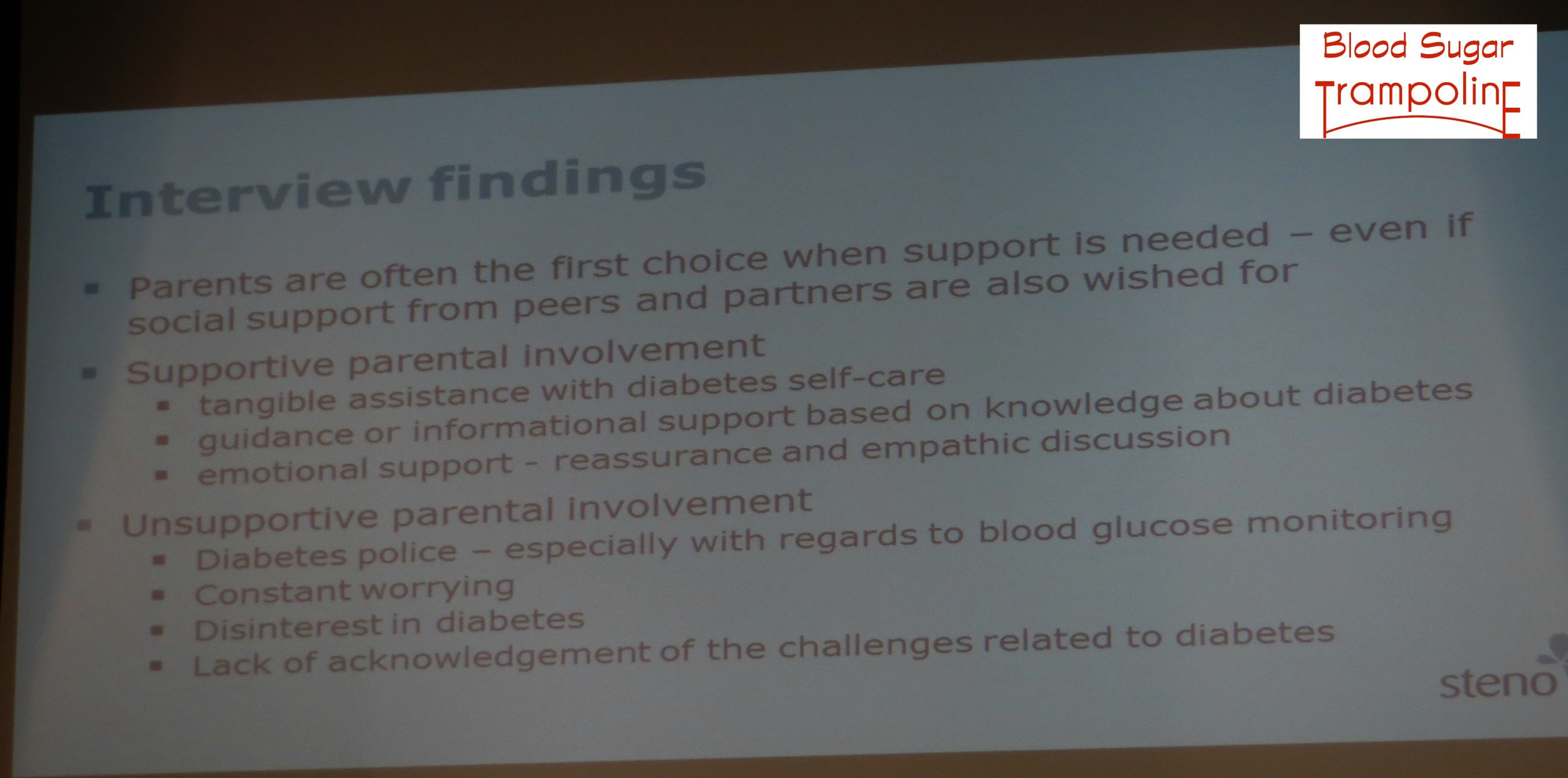 Emerging adults do not want to be too dependent on their parents - they want parents to be available when needed.
Emerging adults do not want to be too dependent on their parents - they want parents to be available when needed.